White Paper
CalAIM: A Mandate and an Opportunity for Transformation
Summary
CalAIM will transform Medi-Cal by integrating it with the state’s broad portfolio of social services. Compliance will require significant investments, challenging cross-functional collaboration, and help from the right healthcare-consulting partner. But CalAIM also offers a unique opportunity to get ahead of the curve as healthcare evolves toward whole-person models for benefits design and management.
By: Mauricio ‘M.J.’ Jimenez, consulting director at Change Healthcare
Maureen Simmonds, MBA, consulting senior manager at Change Healthcare
Executive summary
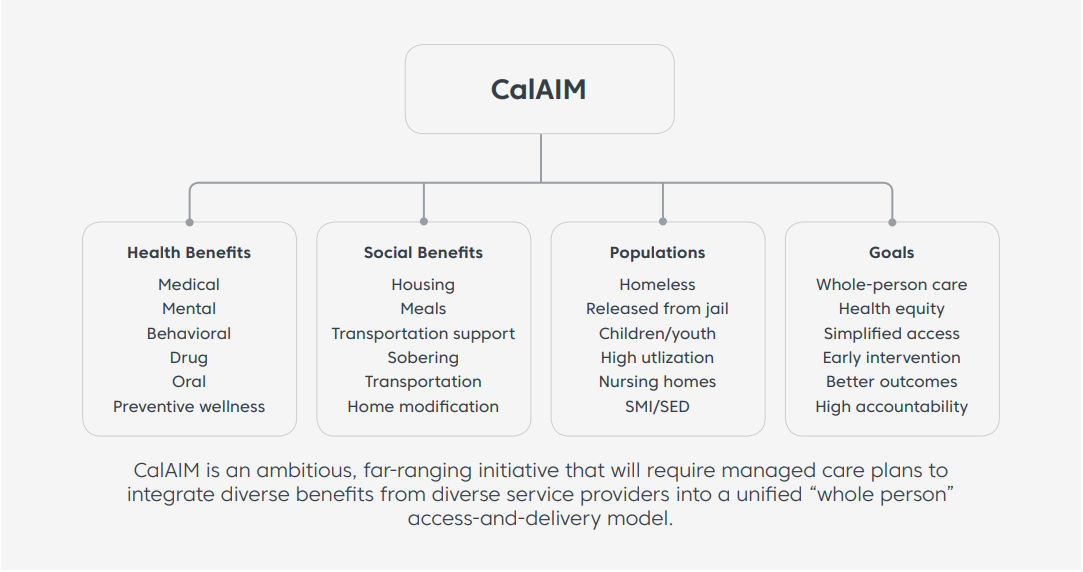
California Advancing and Innovating Medi-Cal (CalAIM) is a far reaching, multiyear plan to transform Medi-Cal by integrating it more seamlessly with the state’s broad portfolio of social services.
The goal: improved outcomes for the millions of Californians covered by Medi-Cal, especially those with the most complex needs.
CalAIM’s core concept is to put the whole person—including their medical, dental, mental, housing, nutritional, and financial needs—at the center of the state’s service delivery.
To achieve this, Department Of Health Care Services (DHCS) will require that all of the current Cal MediConnect (CMC) plans become Medicare Advantage Dual Eligible Special Needs Plans (D-SNPs). These D-SNPs will have integrated care and service and provide eligible members with all of their Medicare benefits, supplemental benefits, D-SNP care, and service, as well as their Medi-Cal benefits and services. Membership in these plans will include dual-eligible members older than 21 who are full-benefit dual-eligible and those who meet low-income levels. These plans will have a unified appeals and grievance process for both Medicare and Medicaid services.
To become a D-SNP, the CMC plans will have to apply to be a Medicare Advantage plan with CMS, file a Part D application for prescription drugs with CMS, and file a Special Needs Plan application with CMS that includes a Model of Care. The Model of Care will define the population to be serviced; the prevalence of clinical and behavioral Social Determinants of Health needs of this population; and the strategy to ensure that each member completes a health assessment, participates in creating an individualized care plan, and has an interdisciplinary care team to support the care plan, their own care manager, and measurable goals. The Model of Care will define the network to serve the population and how the Model of Care will be evaluated annually. CMS will review and process the applications; NCQA will review and score the Model of Care. To implement the D-SNP, there will be major organizational challenges and changes, with new processes, roles, and systems needed to create a successful D-SNP.
Compliance with CalAIM will thus require payers to do much more than merely add coverages here and modify risk adjustments there. It will require a fundamental re-engineering of business rules and workflows across administrative and finance, as well as a breakdown of customer-experience silos.
This compliance challenge will likely be a costly and labor-intensive undertaking that requires significant cross-disciplinary collaboration and external support from the right healthcare-consulting partner.
Executed correctly, however, CalAIM compliance offers payers a unique opportunity to get ahead of the sweeping changes on the horizon as other jurisdictions—and, ultimately, CMS itself—move to whole-person/patient-centric models for the delivery and administration of social benefits.
Organizations facing CalAIM compliance should therefore keep their long-term goals in sight, even as they address the program’s specific requirements and timelines.
What will CalAIM require?
At the heart of CalAIM is the requirement that Medi-Cal managed care plans couple clinical care with a broad portfolio of new, nonmedical services. Those services, which will be reimbursed by Medi-Cal, include housing supports, medical respite, personal care, medically tailored meals, and peer supports.
More specifically, CalAIM specifies:
Next-generation care management
DHCS is proposing a new statewide benefit that it calls “enhanced care management.” This benefit will require an interdisciplinary approach to providing intensive and comprehensive care-management services to clinical and nonclinical circumstances of high-need Medi-Cal beneficiaries. This benefit targets several key populations, including:
- Children and youth with complex physical, behavioral, developmental, and oral health needs (such as those already engaged with California Children’s Services or who have experienced a first episode of psychosis)
- Individuals experiencing homelessness or who are at risk of becoming homeless
- High utilizers with frequent hospital admissions or emergency room visits
- Individuals at risk for institutionalization
- Nursing-facility residents who want to transition to the community
- Individuals transitioning from incarceration who have significant complex physical or behavioral health needs
The new, enhanced care-management benefit builds on the current Health Homes Program and Whole Person Care pilots, which, according to the state, have produced positive outcomes.
Population health management
Under CalAIM, Medi-Cal managed care plans will have to develop and execute patient-centered population-health strategies, which DHCS defines as “a cohesive plan of action for addressing member needs across the continuum of care based on data-driven risk stratification, predictive analytics, and standardized assessment processes.”
Managed care plans will thus, at a minimum, have to define how they will:
- Facilitate preventive and wellness services to keep all members healthy
- Identify and assess member risks and needs on an ongoing basis
- Coordinate care across delivery systems to optimize member outcomes during transitions
- Reduce health inequities by identifying and mitigating Social Determinants of Health
“In Lieu Of” community services and incentives
Building on the success of the Whole Person Care pilot program, DHCS plans to implement “in lieu of” services, which Medi-Cal managed care plans will have to integrate into their population-health strategies.
These services are intended as a substitute—or to avoid—other covered services, such as hospital or nursing-facility admissions. They will likely include:
- Housing/facility transition
- Housing deposits, tenancy, and ongoing support
- Short-term post-hospitalization housing
- Recuperative care (medical respite)
- Personal care and homemaker services
- Home modifications and adaptations
- Meals (including medically tailored diet support)
- Sobering centers
- Asthma remediation
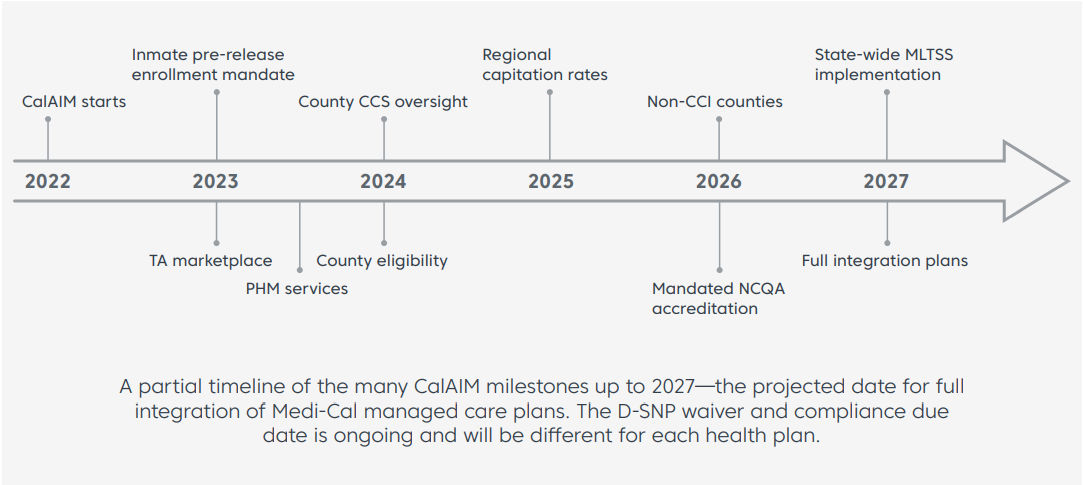
Provision of these wraparound services will initially be voluntary for plans and optional for beneficiaries. However, DHCS is incentivizing plans to integrate managed long-term services and supports (MLTSS) into their managed care program by 2027—with an eye toward building the housing continuum required to meet the needs of the state’s homeless population.
SMI/SED
While federal Medicaid funding generally cannot be used to pay for services provided to a beneficiary while that beneficiary is residing in an Institutional for Mental Disease (IMD), an opportunity has emerged for states to receive federal funding for institutional services provided to populations with a Serious Mental Illness or Serious Emotional Disturbance (SMI/SED)—similar to the flexibility the state has secured for the Drug Medi-Cal Organized Delivery System (DMC-ODS) pilots.
Under CalAIM, DHCS will assess county interest in pursuing the SMI/SED opportunity. Counties would voluntarily “opt in” to participate in a proposed SMI/ SED program that would include:
- Audited care in psychiatric hospitals and residential settings
- Improved care coordination
- Transitions to community-based care
- Increased access to crisis stabilization and other clinically enriched forms of housing in the community
- Earlier identification and treatment resulting from better integration of services
Mandatory enrollment upon release from incarceration
Individuals often receive both medical and behavioral health services while incarcerated in jail or juvenile facilities. Proper coordination is necessary to ensure that the needs of an individual continue to be met upon their release. Also, these individuals often have significant nonclinical needs—such as housing and transportation—as they re-enter their communities.
To ensure that all Californians receive timely access to needed Medi-Cal services upon release from incarceration, DHCS is proposing that the state mandate a prerelease Medi-Cal application process. DHCS is also proposing a mandated process for referrals and links to county specialty mental health, Drug Medi-Cal, DMC-ODS, and Medi-Cal managed care plans for inmates who were receiving such services while incarcerated.
The right partner will help you leverage your CalAIM investments to achieve your broader goals for member care and operational performance.
Fully integrated benefit plans
All of the above specifications are clearly leading to the eventual full integration of physical, behavioral, and oral health under a single contracted entity for each beneficiary. DHCS will clearly have to conduct substantial further research to provide the necessary guidance to managed care plans regarding eligibility criteria, administrative requirements, provider-network requirements, and reporting requirements for quality assurance. Service realignment, the structure of behavioral health under Proposition 30, and other factors also create significant financial complexities for Medi-Cal managed care plans.
Successfully navigating California’s transformation
These proposed mandates have extremely challenging implications for managed care plan providers. Those implications include:
- Intelligently coordinating access to the diverse medical and nonmedical services provided by California’s 58 counties and numerous community-based organizations
- Adapting to payment reforms that drive compensation based on outcomes rather than itemized services
- Being able to demonstrate to the state exactly how the plan has addressed inequities in health outcomes
- Adopting new holistic approaches to risk adjustment, preauthorization, payment accuracy, and other core plan functions
- Minimizing the cost and disruption of reengineering while ensuring timely compliance and optimization results
Given the magnitude of this multidimensional challenge, managed care plan leaders will almost certainly engage with outside consulting and transformation support partners to keep their CalAIM initiatives on track.
Among the key selection criteria for such a transformation partner should be:
A proven record of healthcare-transformation success
CalAIM compliance requires deep expertise in plan operations, budget/financials, and regulatory constraints—as well as experience-won insight into the factors that help determine the success or failure of managed care transformation initiatives.
Strong cross-disciplinary project-coordination skills
CalAIM will require new workflows and process controls across existing organizational silos. The right partner can deliver tremendous value in coordinating these interdepartmental efforts—if that partner intimately understands what every department needs and what risks they must absolutely avoid.
An established commitment to “whole person” care
A CalAIM transformation initiative is no time to engage with a newcomer on the concept of “whole person” care. The ideal supporting partner will therefore already be highly engaged with the industrywide trend toward integrated, outcome-based approaches to administration, access, member communications, and financials.
Essential technical proficiencies
Much of the transformation and cross-disciplinary innovation required for CalAIM centers around technology: data management, analytics, rules-based workflows, digital interfaces with stakeholders, cybersecurity, etc. Your partner should possess the full complement of these critical proficiencies.
Vision for the future
As noted in the Executive Summary, CalAIM presents a unique opportunity to get ahead of the curve as healthcare evolves toward whole-person/patient-centric models for managed care. The right partner will share this vision so your organization leverages its investments in CalAIM compliance to achieve its broader goals for member care, operational performance, and market leadership.
If you’re responsible for your organization’s CalAIM compliance, you have your work cut out for you. The good news is that your work can have truly transformational results for your members, for California’s underserved populations, and for your own organization’s future. Just make sure you get the help you need to achieve those worthy goals.
Key Takeaways
- CalAIM is a bold plan to integrate Medi-Cal with other state services
- To comply, payers must re-engineer and integrate their operational silos
- CalAIM efforts can help payers achieve broader aims for whole-person care


