Case Study
Intelligent Workflow Improves Efficiency and Patient Care
“Being able to carve up the work so there’s accountability and a better level of attention to high clinical priority cases gives us a powerful one-two punch.”
- Dr. Matthew Brady
M.D. Diagnostic Radiologist
Roper Radiologists PA Charleston, SC
Customer
Roper Radiologists PA
Charleston, SC
Challenge
Improving radiologists’ efficiency and contribution to patient care across a radiology practice.
Solution
Change Healthcare Workflow Intelligence
Results
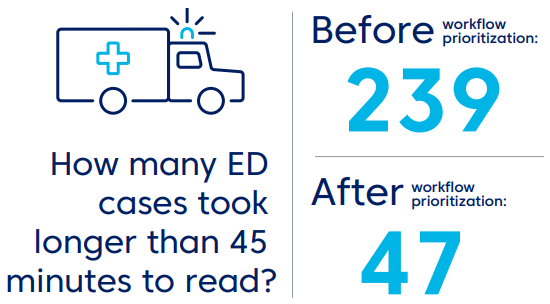
- 56% fewer ED cases slip through the cracks (ones longer than 45 minutes to read)
- 75-minute improvement in average turnaround time (TAT) for outlier studies in the ICU
- 50% fewer ICU studies read after 60 minutes
- 26% less work done after-hours
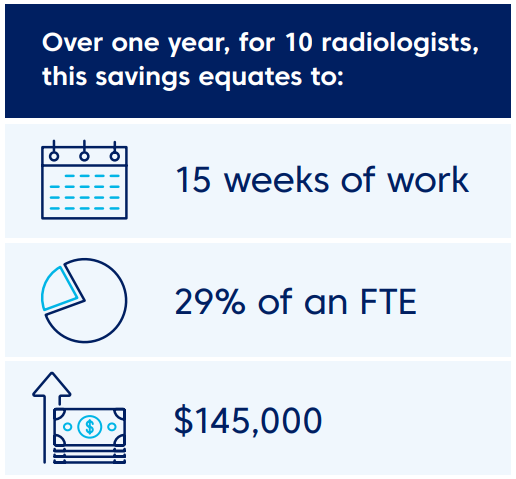
- Accumulated savings add up to 600 hours per year
The Customer:
Roper Radiologists PA is a highly sub-specialized private radiology practice of 25 radiologists in Charleston, South Carolina. They read 300,000 diagnostic imaging studies per year
The Challenge: Improving Efficiency Across A Radiology Practice
"The loss of control over your workday is a problem for any physician no matter what your specialty," says Dr. Matthew Brady, "In radiology, if you're totally disorganized with an unstructured worklist, and you're overwhelmed every day, that's a terrible situation." As radiology workflow becomes increasingly complex, Dr. Brady's practice, Roper Radiologists PA, faced challenges familiar to private groups and hospitals across the country: Distributing and assigning studies, work-life balance, optimizing sub-specialist use, and handling size and volume growth.
To regain control, radiologists at Roper turned first to the traditional filtering capabilities of their PACS worklist, but soon realized its inherent limits. Dr. Brady describes the worklist path as "fraught with pitfalls, unless you have a way to evolve those lists. You see only a certain subset of cases, with no visibility of urgent cases on someone else's list", he says. Another constraint was the lack of sophisticated analytics, which limited the practice's ability to make data-driven adjustments as their workflow changed over time.
The Solution: A Dynamic Worklist Reflects the Practice's Clinical and Operational Priorities
Eventually, the practice separated the concept of diagnostic viewing from workflow management, and searched for a different kind of solution. An interactive, dynamic worklist to orchestrate their workflow and help them measure the results.
They selected Change Healthcare Workflow Intelligence. This flexible rules engine offers a sophisticated prioritization model to manage a complex reading environment. It assigns each study a numbered priority (from 1-99), and then sends studies to the most appropriate and available resource. The solution continually reprioritizes and escalates studies in real time until they're complete. All the data is tracked and time-stamped so it can be analyzed to see what's working and what could be improved.
The solution went live in July 2017, in a process Brady describes as "structured, comprehensive, and smooth," and Roper saw improvements almost immediately.
The Result: Immediate Operational Improvements
Hospitals and radiology practices often use average turnaround times (TAT) as quantifiable benchmarks for improvement. But according to Dr. Brady, "If you look at the math, you'll quickly see that average turnaround times aren't the most useful measurement." Instead, he contends, looking at percentile breakoffs is much more telling. "Percentages, not an average," he says, "because it's inevitable that you end up with long tails - occasional outliers which are read a lot later than the majority."
ED turnaround times are one example that illustrates this situation. Roper's median TAT for ED cases were already excellent; in fact, they read 50 percent of their cases in less than ten minutes and 80 percent of their cases were complete within 22 minutes. But the turnarounds for ED outliers – cases over the 95th percentile – was longer than 49 minutes. And as Brady emphasizes, "Since our median ED turnarounds are extremely short, our median ED may not seem like a big deal. But those are real patients waiting for their results." Roper used the flexible prioritization model to attack these cases, and improved the TAT of these outliers by 17 minutes.
Not only that, but according to Brady, attacking the outliers instead of the average also led to a better relationship with their ED physicians, because it eliminated the recall bias often associated with delayed cases. "No one remembers the 19 cases you read within 15 minutes," he says, "they remember the one that took 45 minutes."
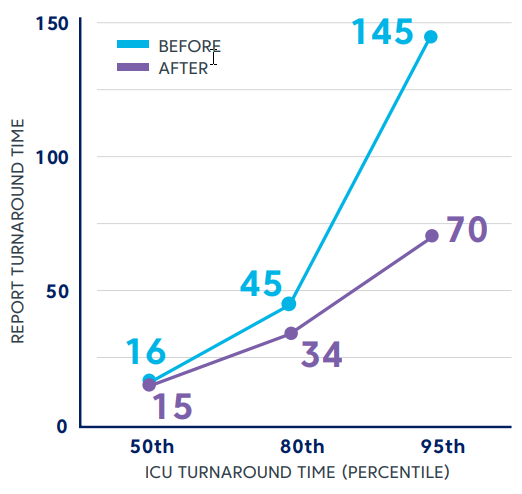
Roper also achieved significant improvements in their ICU turnarounds, including dramatic drops for 80th and 95th percentile cases. In fact, they reduced their TAT for 95th percentile cases by more than half. In Brady's mind, this statistic represents a clear advantage: "The quicker the critical care team has actionable information back in their hands, the better. Being able to differentiate ICU patients from other inpatients is crucial to patient care."
“The quicker the critical care team has actionable information back in their hands, the better. Being able to differentiate ICU patients from other inpatients is crucial to patient care.”
- Dr. Matthew Brady, M.D. Diagnostic Radiologist, Roper Radiologists PA Charleston, SC
It’s important to note that these improvements didn’t come at a cost to other areas. The solution allowed Roper to create ED-specific worklists, which translated into less distractions for radiologists who weren’t assigned to ED studies. This adjustment to their scheduling led to incremental improvements throughout the day which, combined with improved prioritization and more strategic study assignment, created consistent, sustainable change. Some of the results they measured include:
- 56% reduction in ED studies read after 45 mins
- 75-minute improvement in TAT for outlier studies in the ICU
- 50% reduction in ICU studies read after 60 mins
Improving Radiologist Efficiency
Roper began analyzing their data after they deployed Change Healthcare Workflow Intelligence because of an unquantified observation. Dr. Brady thought radiologists were going home earlier, and the analysis proved him right. When Roper examined the number of reports dictated after 5 pm, they confirmed that the amount of work performed by radiologists in the practice dropped by 26%.
Dr. Brady attributes this improvement to the 99 available priority levels that define a study's relative urgency as well as the time limits that determine how and when studies are escalated and distributed. At Roper, ED studies have the most rapid escalation path, with ICU and inpatient studies prioritized less urgently. Dr. Brady describes why this approach works for them, saying, "You read what is your responsibility, but if a case hits a certain threshold, suddenly it appears on everyone's lists and gets dictated very quickly."
When Roper used their PACS worklist to drive their workflow, managing individual profiles and editing individual filters for every radiologist was difficult and time-consuming for their IT staff. Now, lists can be configured at the site-level and adjusted quickly. “Administrators can change a list in thirty seconds, and it’s propagated to everyone,” says Brady. A team of doctors at Roper examined overall volumes and clinical scenarios at the initial stage of the go-live, and established worklists tailored to their specific needs. This ease of administration has fostered a mindset of continuous improvement. “Now, twelve months in,” he states, “we have edited them slightly. The data available from this solution allows us to make this an iterative process. We can see how those lists are working and alter them if we need to.”
Balancing the Workload
Load balancing is a term that's much used and frequently debated. The team at Roper examined the needs of their overall practice and configured rules that emphasized patient care and efficiency. Dr. Brady's advice to anyone considering using a workflow orchestration solution is "not to be constrained by the filters and choices you're used to. You can create any grouping of studies and leverage it to break up the work that you have." At Roper, this meant focusing on distributing work at a macro level instead of adhering to a strictly defined, wRVU-driven model.
The solution enables visibility into workloads, but allows them to achieve balance without micro-managing individual radiologists. The options in Change Healthcare Workflow Intelligence allowed Roper to attack their work differently.
First, they dedicated two FTEs to ED studies. According to Brady, this shift in their practice created "a palpable sense of relief." Before Change Healthcare Workflow Intelligence, he says, "no matter where you were, you always had ED responsibility in the back of your mind. Now, you know exactly when you're responsible for it, which makes your workday a lot more sane."
Brady expects that the solution will continue delivering benefits as they uncover new ways to analyze and use the data, and his goal is to facilitate evidence-based decisions for the practice through ongoing analysis and review. “We’ll have insight over time into our business,” he says. “Having a solution that’s so dynamic and that can be easily edited or changed means we can use the data to evaluate our changes and decisions. For example, staffing and hiring decisions based on data from a product like this one can be more strategically informed. And that’s empowering for the physicians who can control their own work scenario.”


