White Paper
Aligning the Lab With the Hospital’s Strategic Priorities
Summary
Read perspective from Mayo Clinic Laboratory experts and physicians, and dive into proof points from hospital labs that have implemented third-party decision support.
Whitepaper
Ben Gold
Senior Director of Product - CareSelect®, Change Healthcare
Ben Gold drives CareSelect product strategy to enable providers to transition to value-based care. Previously, he worked for Epic managing enterprise EMR implementations for US academic medical centers.
Curtis Hanson, M.D.
Professor of Laboratory Medicine and Pathology, Consultant in Hematopathology, Executive Physician for Healthcare Innovation, Mayo Clinic Laboratories
Curt Hanson, M.D., previously served as chair of the Department of Laboratory Medicine and Pathology and is currently the executive physician for Healthcare Innovation at Mayo Clinic Laboratories. Hanson leads the government relation activities for Mayo Clinic Laboratories, and is the past chair of the board of directors for the American Clinical Laboratory Association.
Introduction
With current events highlighting the critical role of the hospital laboratory as the primary source of diagnostic information and with legislation such as PAMA (Protecting Access to Medicare Act) reducing reimbursements, hospital laboratories must determine the best direction in defining the role of the lab and its value to the healthcare organization.
This white paper is the third in a three-part series developed in collaboration with Mayo Clinic Laboratories and Change Healthcare. The series aims to assist clinical laboratories in understanding the risks and requirements of implementing a clinical decision support (CDS) system in-house versus the benefits of turning to a third-party provider with a proven solution.
This paper provides front-line perspective and commentary from Mayo Clinic Laboratory experts and physicians on the application and value of decision support in the lab. It also includes early-adopter proof points from hospital laboratories that have successfully implemented third-party decision support to achieve their stewardship goals, including electronic health record (EHR) interventions, and ongoing monitoring of utilization.
Two Directions Are Emerging for the Hospital Laboratory
The first option views the lab as a commoditized service and often results in the selling of the hospital lab to a national, at-scale provider such as Quest Diagnostics or LabCorp. In this scenario, economies of scale create a competitive advantage, as do relationships with suppliers of reagents and equipment.
The second alternative involves the creation of a value-based lab that leverages its unique position as a primary source of diagnostic information to influence care delivery. In this scenario, the lab helps drive reductions in cost of care through improved utilization by using data, relationships with clinical leadership, and alignment with organizational strategic priorities to its advantage.
Many of the thought leaders in this second group of hospital labs have identified overutilization and inappropriate lab testing as areas to target for process improvement and cost savings. Applying such improvements would help labs reinvent their role in the organization. Studies estimate that anywhere from 10% to 25%1 of all hospitalperformed laboratory tests in the inpatient setting are not indicated. Unfortunately, the lab’s critical role in determining diagnoses and treatments also makes it vulnerable to abuse.
The blueprint and efficacy of lab test stewardship is well documented as a mechanism to curb overutilization and improve value. To achieve its utilization management goals, a lab test stewardship program requires organizational attention, physician champions, meaningful data, and dedicated IT resources to enact changes. A common element among organizations that have successfully pioneered this path is a partnership with Change Healthcare and deployment of CareSelect Lab.
“It’s the data surveillance and the analytics connected to the guidelines that provides the most value to the organization, which leads to effective stewardship.”
—Don Flott, senior director of Value-Based Medicine, Mayo Clinic Laboratories
Taking Control of Test Utilization Requires Data Analytics
Lab stewardship means true collaboration and partnership between the organization’s clinical leadership and the lab to benefit both. Within a stewardship program, lab expertise expands to inform the medical practice, while the practice utilizes the lab more effectively for the purpose of improving patient care—both clinically and with regards to cost. Most importantly, unlike other efforts that simply focus on making the lab as fast and lean as possible, stewardship has the potential to truly align the lab with the hospital’s strategic priorities.
Defining specific goals and measuring progress towards them requires data. A robust analytics tool integrated with the EHR measures provider behavior against evidence-based guidelines, giving organizations the means to take control of test utilization.
According to Don Flott, senior director of Value- Based Medicine, Mayo Clinic Laboratories, “It’s the data surveillance and the analytics, connected to the guidelines, that provides the most value to the organization, which leads to effective stewardship. You need both. Analytics without clinical standards to support them only tells you what’s common and where you fit among your peers. Analytics backed by standards tells you what you ought to be doing.”
Guidelines created by the Mayo Clinic are being used in a growing number of health organizations around the country. They help to identify the specific lab tests that are most commonly mis-used or over-used by providers. Applying these guidelines are critical for the lab to become an integral part of value-based initiatives in reducing variation and low-value care to improve outcomes.
As providers place lab orders in the EHR, the orders are evaluated for appropriateness in realtime using an integrated surveillance tool, which feeds a robust set of analytics. The information is used to pinpoint locations, departments, and even individual providers that are most frequently placing orders outside of the evidence-based clinical standards from the Mayo Clinic.
A classic example involves a 1,200-bed hospital in the Midwest. The hospital applied the surveillance tool to identify that B-type natriuretic peptide (BNP) was frequently over ordered on their inpatient wards, creating their fourth largest source of inpatient lab waste by spend. This information influenced clinical leadership to turn on a point-oforder alert to warn and inform providers that the test had been recently performed for the patient, and then presented guidance from the Mayo Clinic regarding appropriate use of the test.
In the first month after turning on the alert, the hospital saw a 33% reduction of inappropriate BNP orders. The decline continued, resulting in a 42% drop, on average per month, in inappropriate orders compared to their previous baseline.2
Providers Are Often Making Choices That Are Not Supported by Evidence
With annual direct costs of lab testing in the U.S. estimated at $60 billion, and an estimated 10% to 25% of inpatient tests alone not indicated, waste-related potential savings in the inpatient lab space across the U.S. health system total $6 billion at a minimum.3
Despite general agreement that widespread lowvalue lab testing is generating substantial waste, the potential savings for individual healthcare organizations depends on each organization’s unique situation. Casting a wide net to search for utilization not supported by evidence allows organizations to base stewardship objectives on specific opportunities that offer the greatest impact for financial savings and clinical improvement. It provides the objective evidence necessary to prioritize, motivate, and measure the impact of stewardship efforts.
“When we look at lab data for the organizations we’re working with, we find that a high percentage of opportunity is unpredictable,” says Sean McCormick, M.D., physician informaticist at Change Healthcare. “Although a few guidelines show up on almost every group’s list of those most commonly failed, the majority of an organization’s opportunity is from guidelines that only one or two groups are commonly failing.”
Across an initial base of nine organizations that implemented a core set of Mayo Clinic authored appropriateness guidelines for lab, data showed that almost half of all high-opportunity tests (those with the greatest potential for savings) were unique to only one of the organizations.4
“While provider ordering patterns sometimes differ for good reasons, literature has repeatedly highlighted the fact that providers are often making choices that are not supported by evidence. Our early results have found this to be true as well,” says Dr. McCormick.
Being Responsive to Change in New Tests, Procedures, and Treatments Is a Priority
It’s important for leaders of the lab stewardship effort to take a constructive and clinically grounded approach to their role in reducing unnecessary variation in testing and care delivery in their organization. Medical practitioners operate in a fastpaced, rapidly changing, data-rich environment. An increasingly complex, ever-expanding set of lab test options necessitates a structured, data-driven, scalable approach to lab stewardship.
Early results show that organizations that have implemented the guidelines-informed lab stewardship analytics tool typically find measurable, specific issues to target within the first 60 days of kicking off in surveillance mode.
“The vast majority of physicians are well-meaning, hard-working, informed professionals.” adds Dr. McCormick, “But it is difficult to keep up with the constantly evolving medical literature. New tests, procedures, and therapies are regularly appearing and the strength of evidence for Early results show that organizations that have implemented the guidelines-informed lab stewardship analytics tool typically find measurable, specific issues to target within the first 60 days of kicking off in surveillance mode. Aligning the Lab With the Hospital’s Strategic Priorities 4 them varies considerably. Meanwhile, existing and long-trusted tests and treatments become outdated as new information emerges. Clinically grounded guidelines, applied in an organization that is responsive to change, can help address this dilemma to the benefit of patients and providers.”
Early results show that organizations that have implemented the guidelines-informed lab stewardship analytics tool typically find measurable, specific issues to target within the first 60 days of kicking off in surveillance mode. The most successful organizations have generally seen significant change around targeted utilization issues in the first month after executing interventions to address them.5
Out of the 17 observed organizations that have implemented the tool, most change management interventions are educational or center around order set redesign. Between 5% and 10% of interventions across the customer base are interruptive EHR alerts.6
Although their methods for changing providers’ ordering patterns vary, all have an important element in common: taking action to address the issues they uncover. Implementing a lab stewardship program using evidence-based standards and being driven by data is an organization-wide effort.
“Organizations must realize that even while using advanced analytics to aid in their efforts, lab stewardship is not an IT solution, it’s a medical solution,” says Curt Hanson, M.D., executive physician, Mayo Clinic. “As such, it deserves the attention of clinical leaders at healthcare organizations. And, when applied with an intentional, systematic approach, it rewards that attention with clinical and financial benefits.”
Early Results - Where the Rubber Meets the Road
Following are some early adopter case study results documented by organizations that have implemented a maintained and scalable lab stewardship program founded on evidence-based clinical guidelines. They also applied an analytics and intervention tool integrated with the EHR.
The analytics tool provides:
- A meaningful way to identify waste across the organization. Vetted, evidence-based clinical guidelines help define which orders are appropriate and which are not. Understanding test appropriateness in the context of the patient being seen, and the provider placing the order, is essential to identify areas of waste.
- Access to actionable data that is specific to the organization. Organizations need to understand the current state of lab utilization in order to prioritize, target, and execute interventions that meet their unique challenges with both over- and under-utilization.
- A scalable method to support stewardship goals, including EHR interventions and ongoing monitoring of utilization. Every organization needs to determine how to address the challenges and measure the impact.

Case Study: Hospitals Experience Reduction in Commonly Confused Vitamin D Tests and Send-Outs
There’s money in vitamin D and it’s not just in supplements—though an estimated 75% of Americans take a daily vitamin D supplement. Over a 16-year span, testing vitamin D levels evolved from being relatively rare to mainstream. In 2008, American insurers spent around $1 million on vitamin D tests. Eight years later, they spent $129 million, and by 2016, Medicare patients alone accounted for $365 million worth of testing.7
In a fee-for-service world, the flood of vitamin D testing means more money for the lab—the more tests you perform, the more you get paid. In a valuebased world, what matters more is that the test is appropriate to the clinical scenario, and not all vitamin D tests are equal.
The problem, according to Choosing Wisely: “Many practitioners become confused when ordering a vitamin D test. Because 1,25-dihydroxyvitamin D is the active form of vitamin D, many practitioners think that measuring 1,25-dihydroxyvitamin D is an accurate means to estimate vitamin D stores and test for vitamin D deficiency, which is incorrect.”
https://www.choosingwisely.org/clinician-lists/endocrine-society-vitamin-d-testing/
“Tests that are improperly ordered due to provider confusion are a perfect candidate for intervention by evidence-based CDS,” says Flott. “First, this is because they are obviously inappropriate. Second, running in surveillance mode lets you find where this problem may exist. But it’s the ability to look at the data at the facility level, department level, and at the provider level that is the greatest benefit.”
Being able to evaluate your data and target your actions toward the root of the problem improves the ability to address the problem. 1,25-dihydroxyvitamin D orders coming out of rheumatology or your kidney clinic may be appropriate, while those coming out of family practice may not.
For instance, at one 600-bed hospital on the East Coast that implemented CareSelect Lab as part of their stewardship program, data revealed that a single provider in one family medicine clinic was responsible for 10% of the inappropriate 1,25-dihydroxyvitamin D testing.8
By addressing this one provider’s ordering pattern for inappropriate 1,25-dihydroxyvitamin D testing, the hospital could potentially save money month over month. Then, add the fact that the top three failing providers were responsible for a full quarter of inappropriate orders, and the savings were even greater.9
As Flott notes: “Embracing stewardship is an incremental process. You don’t just find one or two big things to address and then you’re done. It’s an iterative, ongoing process that shows more value the more you progress.”
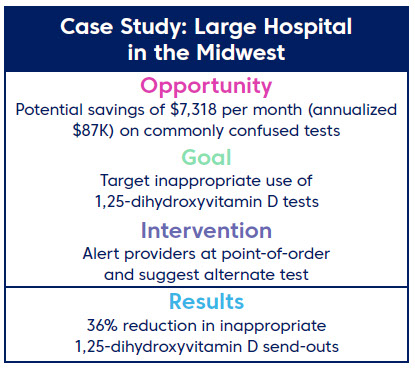
Similarly, a large hospital in the Midwest, which implemented a lab stewardship program based on CareSelect Lab, decided to tackle “commonly confused” tests as the first step in their stewardship program. The first month of data surveillance uncovered that 76% of all orders checked against CareSelect Lab’s commonly confused guidelines failed the check.
As a first step, they decided to tackle 1,25-dihydroxyvitamin D. They set up an alert to warn providers that they were about to order the wrong vitamin D test and proposed an alternative. This measure resulted in a 36% drop in inappropriate 1,25-dihydroxyvitamin D tests across the organization.
This is more impactful then just the drop rate. Since 1,25-dihydroxyvitamin D is a send-out for this organization, a drop in ordering volume is also a drop in the number of send-outs. When you consider that 86% of 1,25-dihydroxyvitamin D were ordered inappropriately, this is significant.
Case Study: Carle Health Improves Order Appropriateness Through Communication and EHR Adjustments
In another case study, Carle Health is a vertically integrated health system with a large physician group, three hospitals with more than 450 beds in the system, and a health plan. Carle’s lab supports both inpatient and outpatient practices.
Carle’s journey to lab utilization started in 2014, when they began compiling data on blood utilization and best practices and adjusted their EHR to implement those practices across the organization.
Within three years, they had built out transfusion best practices and reduced overall blood use by 35% to 40% per 100 patient-bed days. In 2017, they started to address overutilization of inpatient C-difficile PCR testing using the EHR, achieving a 50% reduction in testing.
“It was a good start,” says R. Bruce Wellman, MD, a pathologist and the Medical Director for Transfusion, Coagulation and Apheresis services at Carle Health. “But they needed more. They understood that data, joined to vetted, evidence-based guidelines, would be key to building a successful lab stewardship program.”
“To change provider behavior effectively, you have to understand what is taking place at your institution. You also have to identify which best practices, supported by literature, you want to promote,” Dr. Wellman says.
While Carle had rolled out a few utilization guidelines successfully in their EHR, they struggled with the available databases to get rapid access to the realtime data on their testing activities, which was vital to planning and implementing a broad stewardship program. In 2018, they began working with National Decision Support Company, a Change Healthcare company, to implement CareSelect Lab and focus efforts on low-value testing.
CareSelect Lab gave Carle access to evidence-based guidelines as well as data analytics that helped them decide which undesirable ordering behaviors to target and where and how to target them.
Dr. Wellman points out, “that being able to compare use and misuse by specialty and individual practices and see the variation of ordering practices within specialties lets us target messaging to the areas where interventions can have the biggest impact.”
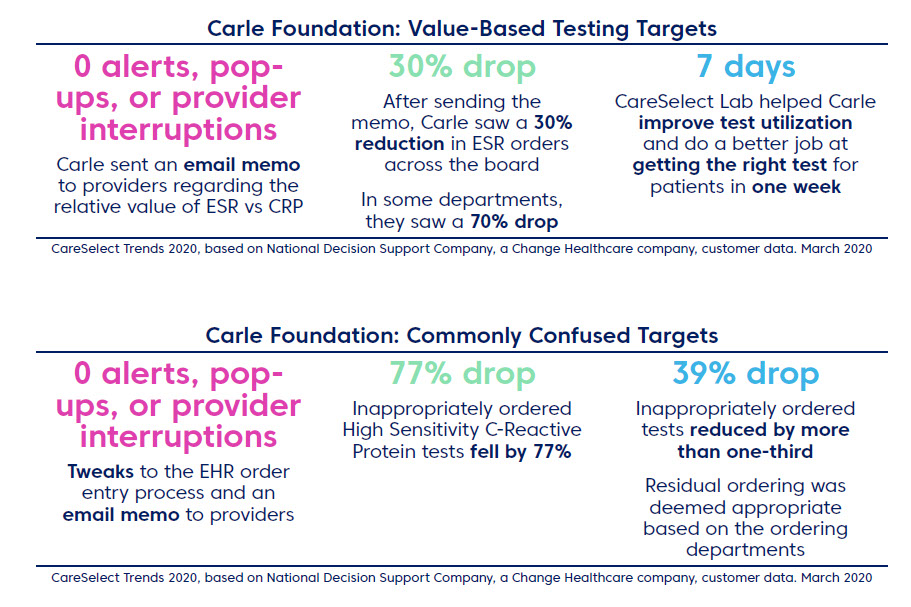
After turning on CareSelect Lab in surveillance mode, Carle analyzed their data. Two items concerning C-Reactive Protein (CRP) orders caught their attention. First, they saw a high failure rate against the commonly confused guideline CRP vs High Sensitivity CRP (HS-CRP). They also saw frequent orders for Erythrocyte Sedimentation Rate (ESR) in scenarios where, according to the Mayo Clinic guidelines used by CareSelect Lab, CRP was a more appropriate test.
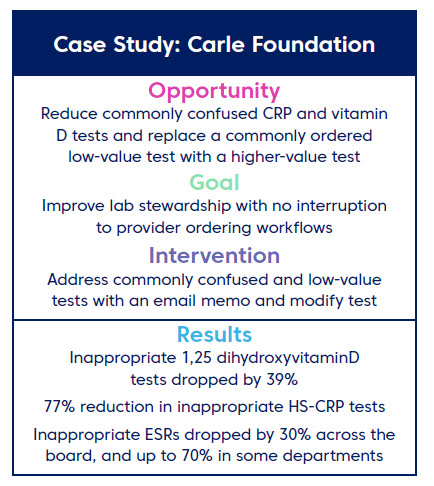
They decided to act on the CRP issues and to address another commonly confused test: 1,25 dihydroxyvitamin D. Since it seemed likely that providers were simply picking the wrong name from a list of search results based on the test name, Carle made changes to the test order names in the search within their EHR. This made it easier for providers to find the test they needed and made it harder for them to confuse tests with similar names.
They addressed the ESR vs. CRP issue with an email memo that showed the guideline against which Carle’s current ordering practices had been evaluated and provided insight about the cost of each test versus actual clinical value. It included details on how much Carle had billed insurance for each test, which in some cases could be denied by the insurer or could get passed on to the patient.
Within one week of making the changes, Carle saw results on all targets, and ordering had dropped dramatically for two of the three tests. Inappropriately ordered 1,25 dihydroxyvitamin D tests were down by 39%, while the HS-CRP orders fell by 77%. They also saw an overall drop of inappropriate ESR orders across the board, falling by as much as 70% in some specialties.
Case Study: Riverside Medical Center Improves Lab Utilization and Reduces Waste
Riverside Medical Center is a 341-bed, short-term acute care hospital in Kankakee, IL. It’s also home to a hospital lab that’s reinventing its relationship to healthcare delivery by demonstrating how the lab can reduce waste and drive value across the organization.
Riverside is accomplishing this by implementing a lab stewardship program using evidence-based clinical decision support. They implemented Epic Beaker in 2016 and saw a resulting decrease in specimen processing times.
“As a lab, we are actively committed to the concept of continuous improvement,” says Stephanie Mitchell, lab director for Riverside. “Adopting Lean methodology in the lab is a long-term, ongoing commitment to quality.”
The success of their previous Lean initiatives caused the lab leadership to be receptive to new approaches and tools that increase the lab’s value to patient care. “It became clear, however, that revamping what happens inside the lab alone isn’t enough to get the lab where it needs to be,” says Mitchell. “We can take on volume without adding resources, but we knew we had opportunities around test utilization.”
“When we saw CareSelect Lab, we knew this could help us improve our test utilization,” says Mitchell. “We liked the analytics that let us look at our data and find opportunities for improvement based on that data. And we were excited by the content, the wide range of vetted guidelines that come ready-made with the tool and that would be maintained for us.”
Riverside had tried to build their own lab-based CDS into the Epic EHR system using the BPA feature, but as Mitchell points out, “The EHR on its own can only go so far. Building our own CDS was incredibly cumbersome.”
They built three guidelines before choosing to move to CareSelect Lab, which offers frequency-related guidelines in the starter set. In May 2019, they turned the tool on in surveillance mode, monitoring orders against a starter set of about 200 guidelines.
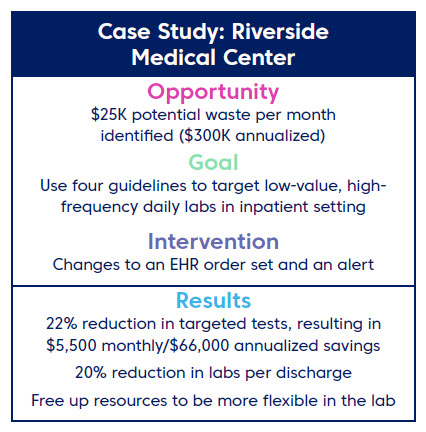
CareSelect Lab exposed almost $25,000 per month in potential savings on lab orders. By adhering to just four frequency rules, Riverside could potentially realize a 27% reduction in monthly waste.
“Once we were able to see some numbers [by running in surveillance mode], we were able to validate our assumptions about utilization issues and zero in on what to target first,” says Mitchell.
They decided to go after the daily labs like the CMP and CBC. They removed default daily lab ordering from their EHR and configured point-oforder feedback to show when a provider places an order for a specific daily test that has already been resulted that day.
Within a month of rolling out their changes, they saw a 22% overall reduction in their targeted tests and a 20% drop in the number of labs per discharge. They also saw some downstream effects both inside and outside of the lab that they hadn’t anticipated from this one intervention.
“Our workflow in the lab has changed,” says Mitchell. “Because the volume of inpatient 5:00 a.m. draws are down, we’ve been able to rethink how we use our staff in the mornings. We can be more flexible with work assignments and scheduling.”
Outside of the lab, the success of their first pass at stewardship has reinforced enthusiasm for the project across the organization. “It was important to show our leadership specific examples of where the potential was,” says Mitchell. “Just as importantly, the physicians like it. They appreciate that we’ll be able to help them order the right test.”
Conclusion – Decision Support Is Vital to Driving a Strategic Stewardship Initiative
Early adopter results, as outlined in this white paper, confirm that clinical decision support tools such as CareSelect Lab, which merge evidence-based guidelines and strong analytics, can help hospital laboratories implement stewardship programs with proven results.
Hospital laboratories that have implemented CareSelect Lab as part of a strategic stewardship initiative found a specific issue to target within the first 60 days of data collection. They saw a measurable improvement in the targeted issue within a month of intervention, with associated financial savings and beneficial downstream effects that leave them better positioned to take advantage of outreach and other opportunities.
They also had an impact on test utilization without adversely impacting clinicians or care. Approximately 90% of successful interventions were non-interruptive to clinician workflows. In addition, patients were more likely to get the correct diagnostic test and less likely to receive an unnecessary test as a result of point-of-order CDS.
CareSelect Lab, developed by National Decision Support Company, a Change Healthcare Company, is a decision support tool that integrates with leading EHR solutions and aggregates clinical knowledge around a select menu of routine conditions, then translates that knowledge into maintained medical policies and best-practice recommendations.
It is unique in that its underlying clinical guidance includes more than 1,800 best practice rules authored, curated, and maintained by Mayo Clinic physicians and scientists. The guidelines are grounded in evidence-based research, industry best practices, and vetted Mayo Clinic policies and procedures. They collectively constitute one of the most comprehensive and detailed set of evidence-based tools for clinical laboratory testing available today.
Download the first white paper or audio book “Industry Report: Clinical Laboratories at a Crossroads – Hospitals must choose best path forward amid major industry changes.”
https://www.changehealthcare.com/resources/detail/clinical-laboratories-at-a-crossroads
Download the second white paper or audio book “Reality Check: Buy Versus Build for Laboratory Decision Support – Hospital Laboratories Must Think Critically and Evaluate Carefully Before Launching Decision Support Projects.”
https://www.changehealthcare.com/resources/detail/lab-decision-support-buy-versus-build
1 Based on National Decision Support Company, a Change Healthcare company, CareSelect Lab customer data, November 2019
2 Based on National Decision Support Company, a Change Healthcare company, CareSelect Lab customer data, November 2019.
3 Am J Clinical Pathology. 2013;139(1289-1297)
4 Based on National Decision Support Company, a Change Healthcare company, CareSelect Lab customer data, March 2020
5 Based on National Decision Support Company, a Change Healthcare company, CareSelect Lab customer data, March 2020
6 Based on National Decision Support Company, a Change Healthcare company, CareSelect Lab customer data, March 2020
7 Kaiser Health News, The Man Who Sold America on Vitamin D and Profited in the Process, August 2018 and, Julia Belluz, Vox.com, Why vitamin D has the medical establishment totally confused, December 2014
8 Based on National Decision Support Company, a Change Healthcare company, CareSelect Lab customer data, March 2020
9 Based on National Decision Support Company, a Change Healthcare company, CareSelect Lab customer data, March 2020
10 Interview with Stephanie Mitchell, Lab Director, Riverside Medical Center


