White Paper
Education is Key to Improving Provider E/M Coding Accuracy
Summary
Did you know that approximately 94% of physician billing errors are simply mistakes?
Executive Summary
Errors in physician coding cost billions of dollars each year to the U.S. healthcare system. Such a large financial impact can be attributed to a relatively small problem: human error. This white paper delves into the details surrounding the problem, and shares a simple solution.
It’s no secret that today’s healthcare environment is undergoing massive changes. There are a multitude of initiatives transforming the current healthcare landscape as we know it, including the Affordable Care Act, health exchanges, corporate-based wellness and population health management, Accountable Care Organizations, medical homes, and consumer-driven healthcare.
The list of acronyms and need for “new thinking” is daunting. Most, if not all, of these initiatives are rooted in sound principles, unique in their own way, and by and large have positive impacts on the quality and costs of specific aspects of healthcare delivery. At their core, they seek to solve the same underlying (and enormous) problem: skyrocketing healthcare costs. Estimated to be 17.8% of the GDP in 20151, healthcare in the United States has the highest measurable costs in the world. The current trajectory is not sustainable, and, at the risk of stating the obvious, healthcare must be redefined.
While this may seem insurmountable, it doesn’t have to be. Providers, payers, partners, and even consumers do not need to “eat the elephant in one bite,” so to speak. All around us there are meaningful, effective, actionable ways to reduce healthcare costs. One example is to address the high cost of inaccurate coding/ billing, which leads to overpayment of claims.
E/M Coding Issues Gain Prominence through OIG and Medicare
The area of physician billing is largely unregulated and mired with inefficiencies and inaccuracies that result in billions of dollars of inappropriate payments to physicians. This issue garnered national attention in May 2012 when the Office of Inspector General (OIG) issued a report stating that between 2001 and 2010, Medicare payments increased by 43 percent, from $77 billion to $110 billion.
During this same period, Medicare payments for evaluation and management (E/M) services increased by 48 percent, from $22.7 billion to $33.5 billion. This $11 billion increase in payments over ten years includes a 13 percent increase in the number of E/M services billed, 346 million to 392 million. The payment amount increased 31 percent, from $65 to $85 per visit.2
The OIG reports E/M services are 50% more likely to be paid in error than other Part B Medicare services.3
The OIG worked with CMS to conduct an analysis of physicians’ E/M claims using Part B Medicare claims. As a result of the analysis, the OIG “identified approximately 1,700 physicians who consistently billed higher level E/M codes in 2010 [known as “high-coding physicians”]. Although these physicians differed from others in their billing of E/M codes, they practiced in nearly all states, and represented similar specialties. The physicians who consistently billed higher level E/M codes also treated beneficiaries of similar ages and with similar” diagnoses as those treated by other physicians.2
In 2014, the OIG reported findings from its 2010 claims review of CMS payments for E/M services: 55 percent of all E/M claims were incorrectly coded and/or lacked documentation, resulting in $6.7 billion in inappropriate payments.3
2010 OIG Summary3: Medicare Payment for Evaluation and Management (E/M) Services
- $32.2 billion total
- $6.7 billion (21 percent of total payments) was inappropriately paid
Of the Inappropriately Paid Claims:
- 55% were incorrectly coded and/or lacked documentation. Of these:
- 26% were upcoded
- 15% were downcoded
- 2% included wrong codes (non E/M, unbundled, etc.)
- 12% included insufficient documentation
- 7% were undocumented
- 6.7% overlap of incorrect coding and lack of documentation
After completing the analysis, the OIG recommended the following actions to CMS:
- Educate physicians on coding and documentation requirements for E/M services
- Continue to encourage contractors to review E/M services billed for by high-coding physicians
- Follow up on claims for E/M services that were paid for in error
Root Cause Behind Inaccurate Billing: Simple Human Error
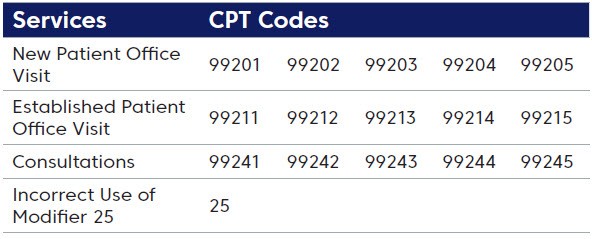
While one’s first inclination may be to assume coding inaccuracies on low-dollar, high-volume claims are due to fraudulent billing practices, in reality this is rarely the case. In a recent study conducted by Change Healthcare, the breakout for coding inaccuracies was primarily due to simple billing errors. The following services and CPT codes were the most often mis-coded services:
Further, Change Healthcare found that billing errors seemed to be attributed primarily to three key factors:
- Little to No Regulation: Because physician billing is unregulated, there are no hard and fast disciplines for billing, which allows various interpretations and methods to be practiced.
- Electronic Medical Records Systems: With EMR systems now mainstream, physicians and billing staff can produce detailed records and complete billing quickly, with no real audit measures in place to detect multiple clicks or inaccurate charges on a consistent basis.
- Education: The majority of physicians fully believe they are appropriately and correctly billing for services provided; there is rarely any intention to upcharge or mischarge for services. Rather, a lack of education and training is the root cause of their errors.
Root Causes in Low-Dollar, High- Volume Coding Inaccuracies
- Billing errors (94%)
- Abusive billing (5-6%)
- Fraudulent billing (<1%)
Reduce Billing Aberrancies
Both the OIG report and the Change Healthcare study indicate the key to reducing E/M coding errors is educating physicians and their billing staff. Since the majority (94%*) of these errors are simple mistakes, increasing awareness and working to change ingrained behaviors can produce significant results. The Change Healthcare Coding Advisor solution uses a four-phase approach:
- Identify outlier providers
- Educate providers and billing staff to help them understand coding requirements and modify their behavior
- Validate that coding errors have been reduced or eliminated
- Act if providers fail to make improvements.
Real Savings
The first client to implement Coding Advisor achieved significant results in its first year, with Change Healthcare reviewing 241,000 physicians and reducing payments by $27 million. The population base was then expanded and produced similar results; the client soon expects to reach $40 million in cumulative savings. Coding Advisor is now being used to help numerous payers reduce overpayments of low-dollar, high-volume claims.

One Solution at a Time
Change is the one constant in life, and that is certainly true for the healthcare industry. Fortunately, with change comes opportunity. Change Healthcare can help you leverage that opportunity for success. To learn more about how Change Healthcare enables smarter healthcare, visit changehealthcare.com.
1 Centers for Medicare and Medicaid, cms.gov/research-statistics-data-and-systems/statistics-trends-and-reports/nationalhealthexpenddata/ nationalhealthaccountshistorical.html
2 Department of Health and Human Services, Office of Inspector General, Coding Trends of Medicare Evaluation and Management Services, Daniel R. Levinson, May 2012 http://oig.hhs.gov/oei/reports/oei-04-10-00180.pdf
3 Department of Health and Human Services, Office of Inspector General, Improper Payments for Evaluation and Management Services Cost Medicare Billions in 2010, Daniel R. Levinson, May 2014 https://oig.hhs.gov/oei/reports/oei-04-10-00181.pdf
*Change Healthcare study


